What is Huntington's Disease?
Late onset Huntington's disease is an autosomal dominant genetic disorder that affects the central nervous system of human beings. This disease typically shows up when a person reaches their mid 30's or 40's, with no earlier signs or symptoms. The nerve cells of an affected individual quickly degenerate in certain parts of the brain, which leads to symptoms that include dementia, loss of memory, and severely decreased mental capacity, muscle rigidity, and loss of bodily function and muscle coordination. Huntington's usually shortens an affected persons lifespan, with the average person dying 15-20 years after onset of the disease, making the life expectancy around 50-60 years of age, but suicide is common before that point.

|
|
How are genetics involved?
Huntington's disease results from a genetic defect on the autosomal chromosome number 4. The specific gene pair that is affected is named the Huntingtin gene. The term autosomal refers to the 22 chromosome pairs that are not the sex chromosomes, so this means that Huntington's can affect men and women equally. The trait is dominant, which means that the defective"bad" gene on one chromosome expresses itself more strongly than the "normal" properly functioning gene on the other chromosome.
What are my odds of having Huntington's and passing on the trait?
Family history plays a very important role in the inheritance patterns of autosomal dominant disorders. In Huntington's diseases if one of you're parents has been diagnosed with Huntington's disease you have a 50% chance of receiving the defective gene from that parent. If both of your parents have Huntington's disease the odds of receiving a defective gene increase to 75%. If you do have the disease, the odds for you passing the trait onto your children would be the same as listed above, 50%.
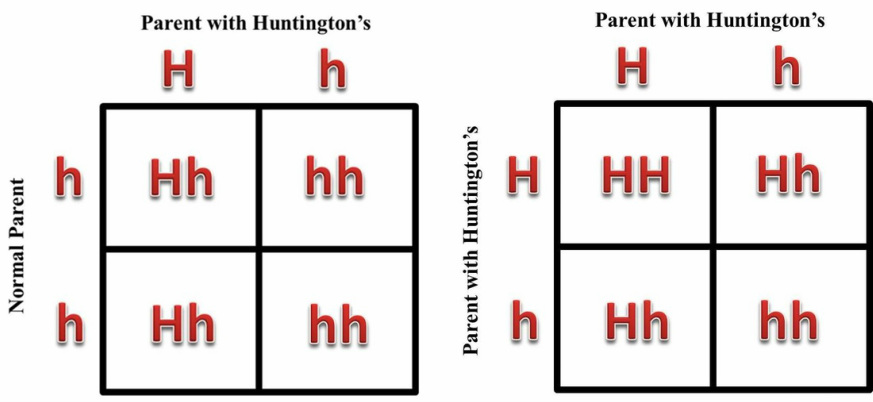
A simple Punnets square shows the possible outcomes for each child that you would birth in both scenarios. A Punnet square is a simple figure that shows all of the possible gametes from a parent and shows all of the possible outcomes from the potential children being born to that set of parents. This disorder consists of two alleles for the Huntingtin gene, a big H (Dominant) and a little h (Recessive). Alleles are simply the two different forms that the Huntingtin gene can take on. Dominant simply means any genotype that is physically represented in a heterozygote (Hh). Recessive means that the trait is hidden in the heterozygote. Since Huntington's disease is dominant, the gene responsible for the disease will be represented by a big "H" while the normal gene is represented by a small "h". Any child having a big "H" will inherit the disease any child with the genotype "HH" will most likely not survive to birth. Having the "hh" genotype means that the child is normal and does not inherit the disease.
A simple Punnets square shows the possible outcomes for each child that you would birth in both scenarios. A Punnet square is a simple figure that shows all of the possible gametes from a parent and shows all of the possible outcomes from the potential children being born to that set of parents. This disorder consists of two alleles for the Huntingtin gene, a big H (Dominant) and a little h (Recessive). Alleles are simply the two different forms that the Huntingtin gene can take on. Dominant simply means any genotype that is physically represented in a heterozygote (Hh). Recessive means that the trait is hidden in the heterozygote. Since Huntington's disease is dominant, the gene responsible for the disease will be represented by a big "H" while the normal gene is represented by a small "h". Any child having a big "H" will inherit the disease any child with the genotype "HH" will most likely not survive to birth. Having the "hh" genotype means that the child is normal and does not inherit the disease.
While the Punnet square shows the cross of two individuals, another way to look at family history is through Pedigree analysis. A pedigree effectively shows which individuals had/have the disease and whether or not their children received the defective gene. Since Huntington's disease is dominant it is either present in every generation or will disappear from a family history after a generation that avoids receiving the gene. Here is an example of three generations of a family with Huntington's disease:
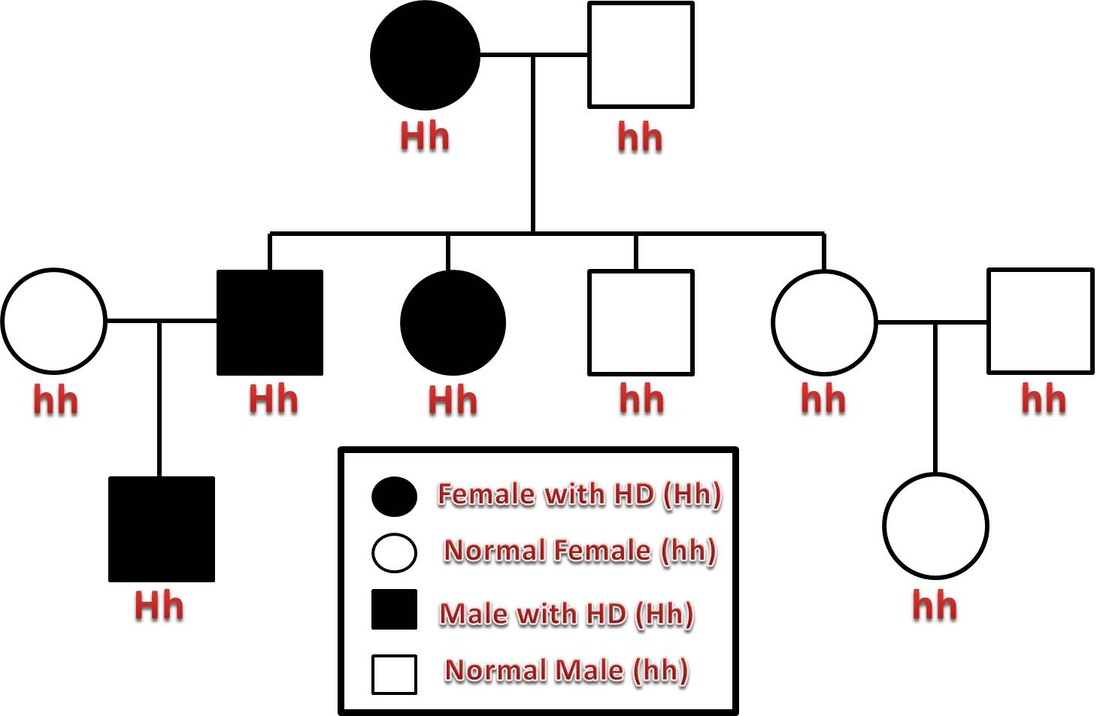
In this example pedigree the first generation resulted in a cross between a woman with Huntington's Disease and an unaffected male. 50% percent of their children, in the second generation ended up getting the "bad" dominant allele for Huntington's. Only the second generation individuals will have the possibility of passing of the bad allele to their children, which is evident in the left side of the pedigree chart.
Genetic Testing
There are several ways of testing for the presence of the bad gene that causes Huntington's disease. A couple with a family history of Huntington's disease may wish to undergo prenatal testing, which checks both potential parents for the presence of the Dominant allele. This can then give the parents a good idea of what their chance of having a child with Huntington's is. If both parents are homozygous recessive (hh) for Huntington's, then they would have a 0% chance of having a child with the disease. If one parent has the Dominant allele, they have a 50% chance of having a child that will develop Huntington's disease. This then lets the parents weigh their options on whether to have a child or possibly adopt and forgo the risk.
If the pregnancy has already started and the parents want to know whether the developing fetus has the disorder Chronic Villus Sampling (CVS) can be done around 10 or 12 weeks of development. CVS consists of taking a biopsy of part of the placenta that surrounds the fetus which can be risky to the developing child.
These choices normally involve consulting with a certified genetic counselor who will lay out the risk and benefits of all testing options. The counselor will also give you testing options based on your family history.
If the pregnancy has already started and the parents want to know whether the developing fetus has the disorder Chronic Villus Sampling (CVS) can be done around 10 or 12 weeks of development. CVS consists of taking a biopsy of part of the placenta that surrounds the fetus which can be risky to the developing child.
These choices normally involve consulting with a certified genetic counselor who will lay out the risk and benefits of all testing options. The counselor will also give you testing options based on your family history.

Treatment Options for Huntington's Disease
There is currently no cure for Huntington's and the resulting effects of the disease are devastating for the individual with the disease and their families. There is also no treatment for delaying the onset of the disease so the intended goal for treatment is to alleviate the symptoms associated with the disease. Dopamine blockers are used to stop uncontrolled movements and abnormal behaviors. Amantadine and tetrabenazine are drugs currently being used to try to control extra movements. Physical therapy and occupational therapy are also used to help try and maintain some muscular function. It needs to be understood that individuals with Huntington's will decline in health rather quickly upon onset of the disease. These individuals will need to need assistance and supervision, which will eventually be needed 24 hours a day, 7 days a week. People with Huntington's usually die from infections not related form the disease such as pneumonia and other infections.

References
1. "Chorionic Villus Sampling (CVS)." WebMD. HealthWise, 06 May 2010. Web. 19 Sept. 2012. <http://www.webmd.com/baby/chorionic-villus-sampling-cvs>.
2. Clain, John. "Know Symptoms of Huntington's Disease for Treatment." B4Tea. Blogspot, 2011. Web. 19 Sept. 2012. <http://b4tea.blogspot.com/2012/02/know-symptoms-of-huntingtons-disease.html>.
3. Collins, Debra. "Genetics of Huntington Disease." Genetics of Huntington's Disease. University of Kansas Medical Center, 15 Feb. 1999. Web. 16 Sept. 2012. <http://www.kumc.edu/hospital/huntingtons/genetics.html>.
4. "Huntington's Disease (HD). " Huntington's Disease (HD). Interactive Health, LLC., n.d. Web. 19 Sept. 2012. <http://iahealth.net/huntingtons-disease/>.
5. "Huntington's Disease." Pub Med Health. U.S. National Library of Medicine, 30 Apr. 2011. Web. 15 Sept. 2012. <http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001775/>.
6. "The Kobiljak Centers." Kobiljack Centers. Michigan State University School of Medicine, 6 May 2012. Web. 15 Sept. 2012. <http://kobiljak.msu.edu/>.
2. Clain, John. "Know Symptoms of Huntington's Disease for Treatment." B4Tea. Blogspot, 2011. Web. 19 Sept. 2012. <http://b4tea.blogspot.com/2012/02/know-symptoms-of-huntingtons-disease.html>.
3. Collins, Debra. "Genetics of Huntington Disease." Genetics of Huntington's Disease. University of Kansas Medical Center, 15 Feb. 1999. Web. 16 Sept. 2012. <http://www.kumc.edu/hospital/huntingtons/genetics.html>.
4. "Huntington's Disease (HD). " Huntington's Disease (HD). Interactive Health, LLC., n.d. Web. 19 Sept. 2012. <http://iahealth.net/huntingtons-disease/>.
5. "Huntington's Disease." Pub Med Health. U.S. National Library of Medicine, 30 Apr. 2011. Web. 15 Sept. 2012. <http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001775/>.
6. "The Kobiljak Centers." Kobiljack Centers. Michigan State University School of Medicine, 6 May 2012. Web. 15 Sept. 2012. <http://kobiljak.msu.edu/>.
